Increasing incidence of pancreatic cancer
The urgent need for improvements in diagnostics and therapy, especially for pancreatic cancer, is now underlined by a current international study on the worldwide development of the tumor.
Lifestyle as the most important risk factor
Pancreatic carcinoma has almost traditionally been one of the problem children of gastroenterology and oncology. So far, there are no effective new therapies that would significantly reduce mortality from this tumor, which is often discovered late. The urgent need for improvements in the fields of diagnostics and therapy, especially for pancreatic cancer, is now underlined by a current international study on the worldwide development of the tumor.1 The incidence and mortality are rising particularly among women and people aged 50 and over, but also among younger people.1 The study evaluated data from high-quality cancer registries from 48 countries for the reference year 2018.
Pancreatic cancer is the 12th most common cancer worldwide, but ranks seventh in terms of mortality.2 This marked discrepancy reflects the aggressive nature of pancreatic cancer and the generally poor survival prospects of patients. Together with widespread difficulties in diagnosis and the tendency towards low response to radiological and chemotherapeutic treatment attempts, they form the background to the high mortality from the disease.
In addition to unchangeable factors (age, gender, ethnic background, familial and hereditary burden), lifestyle has been identified as the main risk factor. Smoking, physical inactivity, obesity, hypertension, diabetes mellitus, hypercholesterolaemia, chronic pancreatitis and exposure to specific chemicals increase the risk of disease.3
According to the study, nearly 459,000 new cases of pancreatic cancer occurred worldwide in 2018, compared to just over 432,000 deaths from the disease. The age-standardised incidence was thus 4.8 per 100,000 inhabitants worldwide, with considerable regional variation (10.8 per 100,000 for Hungary, 0.35 per 100,000 for Guinea). In particular, countries and regions with a high standard of living such as North America, Western and Central Europe as well as Eastern Europe showed high incidences (cf. Fig. 1 and 2).
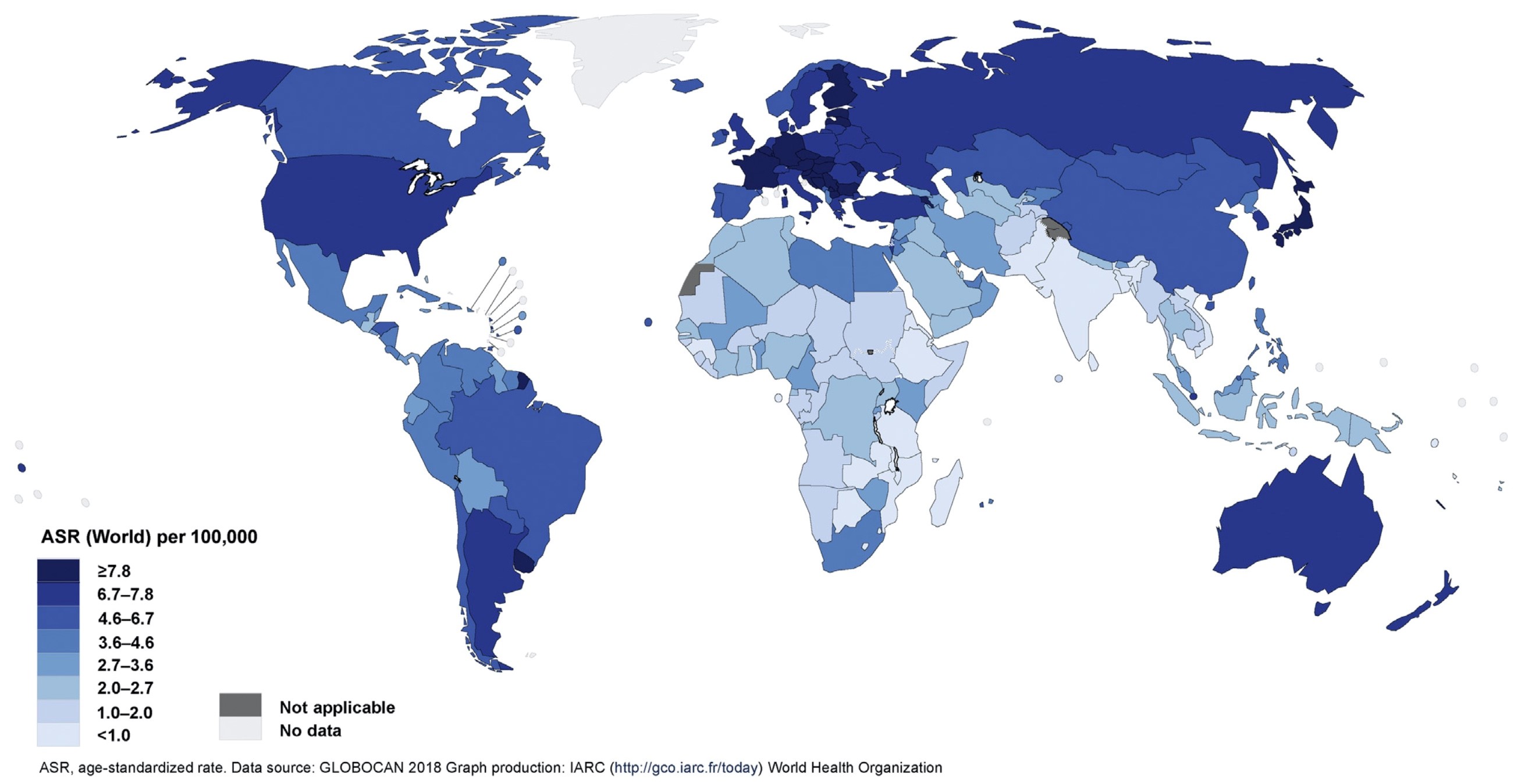
Fig. 1: Worldwide age-standardised (ASR) incidence of pancreatic cancer (according to [1]).
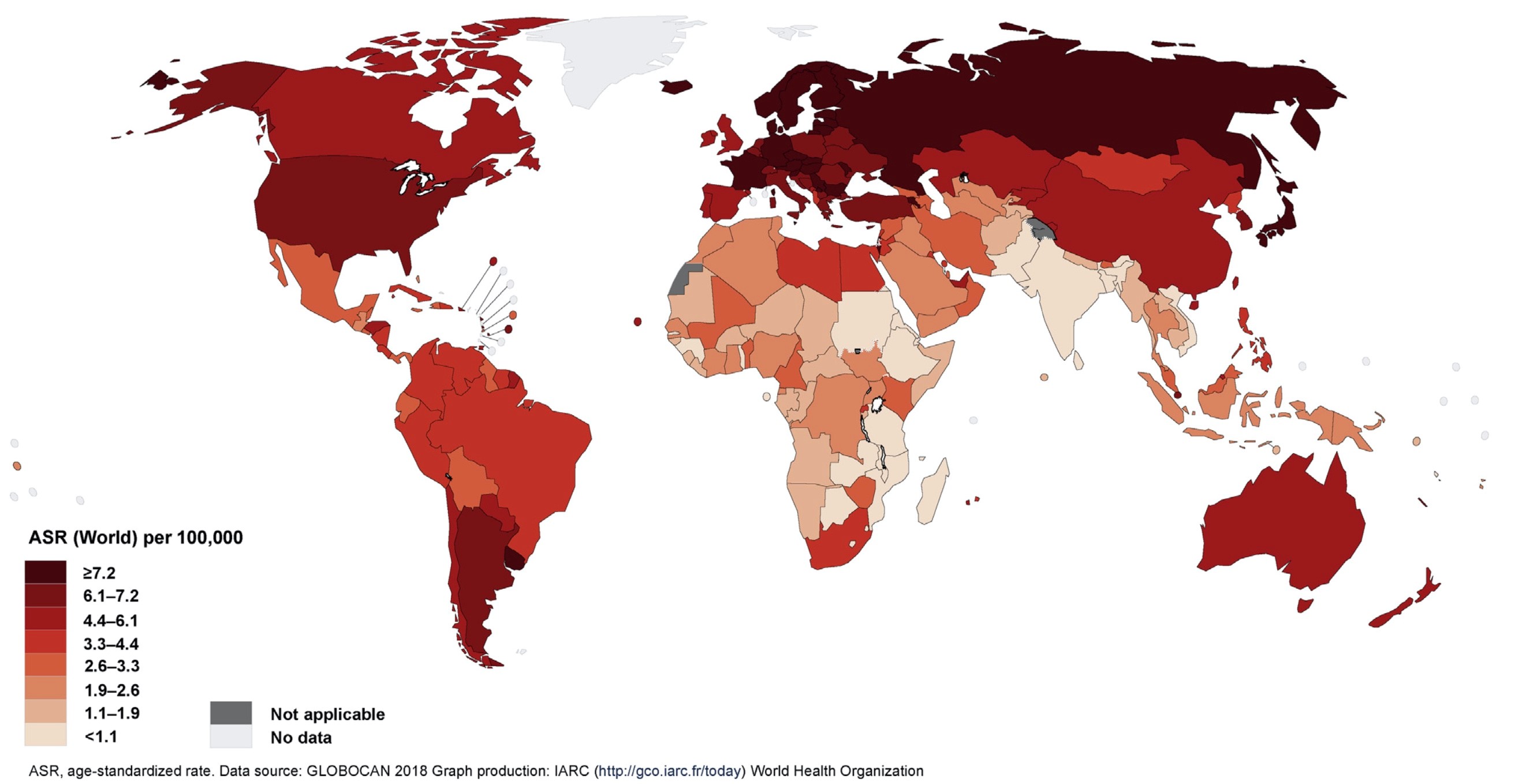
Fig. 2: Worldwide age-standardised (ASR) mortality of pancreatic cancer (according to [1]).
Compared to the previous survey, which took place about a decade ago4, different developments became apparent:
- Especially among women and older people, both the incidence and mortality of pancreatic cancer increased. According to the authors, this could be an expression of the increase in the prevalence of the particularly relevant risk factor of overweight in the populations of the countries studied, which is increasing even faster among women than in the general population.
- There is a trend towards the occurrence of pancreatic carcinomas before the age of 50. The authors also blame the increase in overweight among younger people for this observation.
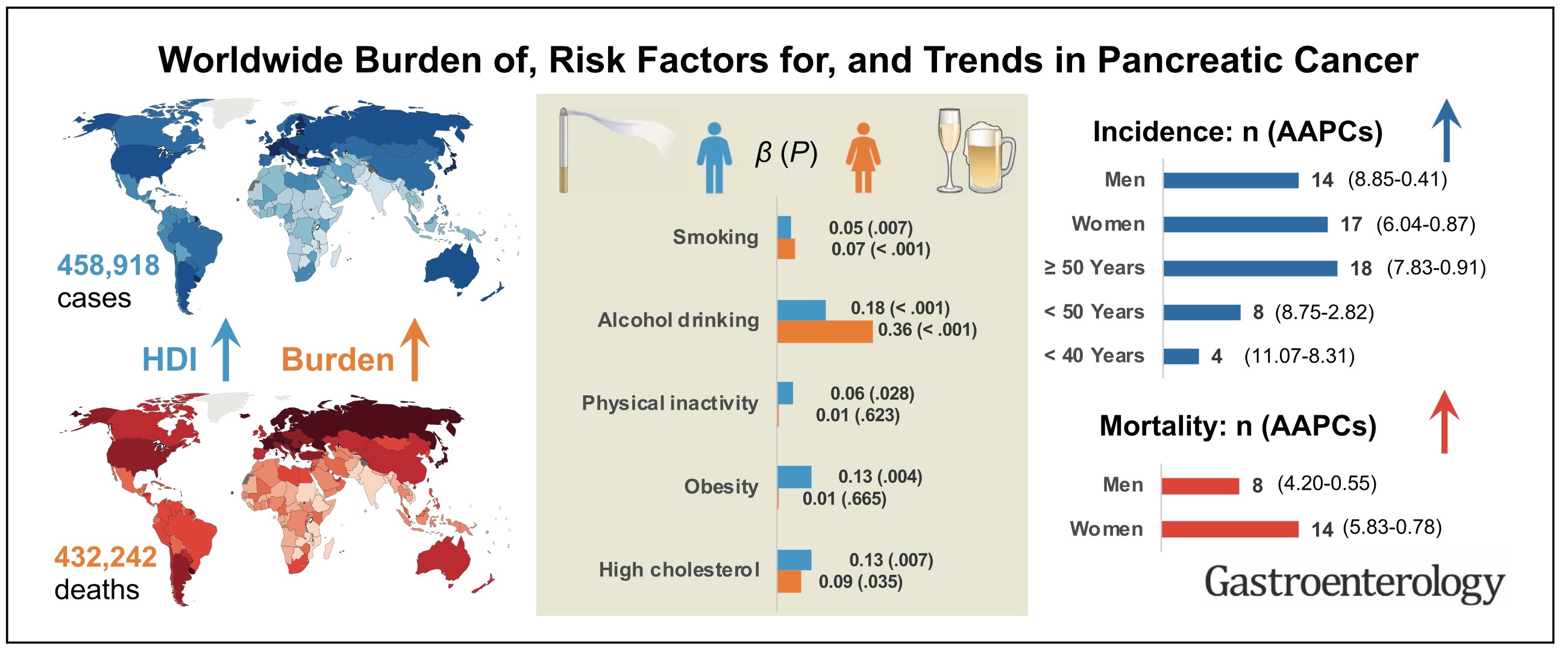
Fig. 3: Graphical summary of the main results of the study presented (according to [1]). HDI: Human Development Index (measure of a country's level of development); AAPC: Average annual percentage change.
In view of the worrying results of their study (cf. graphical representation in Fig. 3), the authors call for increased efforts to enable and ensure early diagnosis and effective treatment of pancreatic cancer.
References:
1. Huang J, et al. Worldwide Burden of, Risk Factors for, and Trends in Pancreatic Cancer. Gastroenterology 2021; 160: 744-754. https://www.gastrojournal.org/action/showPdf?pii=S0016-5085%2820%2935244-6
2. Bray F, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394-424. https://acsjournals.onlinelibrary.wiley.com/doi/full/10.3322/caac.21492
3. Midha S, Chawla S, Garg PK. Modifiable and non-modifiable risk factors for pancreatic cancer:A review. Cancer Lett 2016; 381: 269-277. http://refhub.elsevier.com/S0016-5085(20)35244-6/sref6
4. Maisonneuve P, Lowenfels AB. Epidemiology of pancreatic cancer:an update. Dig Dis 2010; 28: 645-656. https://www.karger.com/Article/Abstract/320068